What is shoulder impingement?
Shoulder impingement, or shoulder impingement syndrome, is a very common cause of shoulder pain, where the supraspinatus tendon (one of the rotator cuff tendons) inside your shoulder joint rubs or catches on nearby tissue (bursa) and bone (acromion) as you lift your arm.
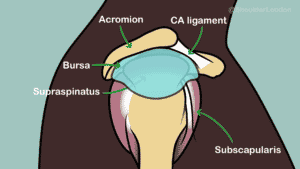
Side view of normal anatomy of the shoulder. (Click to enlarge)
Shoulder impingement is an old term that gave the impression that all pain in this region was caused by the rotator cuff tendon and bursa being pinched between the humeral head and acromion and we now realise that this is an oversimplification, and that pain can happen with no mechanical problem, so pain in this region is now referred to as Subacromial Shoulder Pain.
Shoulder impingement is just one of the causes of subacromial shoulder pain. The other causes of subacromial shoulder pain include rotator cuff tendinopathy, partial thickness rotator cuff tears, subacromial bursitis and calcific tendonitis.
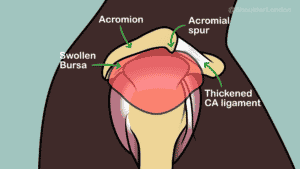
Side view of shoulder showing acromion spur, thickened CA ligament, and swollen bursa (CLick to enlarge)
True shoulder impingement is rare. In patients with shoulder impingement there is often a bony spur on the acromion with thickening of the coracoacromial ligament. These combined reduce the space for the rotator cuff tendon to glide as the arm is lifted. Patients with shoulder impingement often also have rotator cuff tendinopathy and can have subacromial bursitis as well.
What are the symptoms of shoulder impingement?
Shoulder impingement is usually a condition that has gradual onset. Patients mostly complain of pain on the outside of the shoulder over the deltoid muscle. Symptoms include:
pain in the top and outer side of your shoulder
pain that’s worse when you lift your arm, especially when you lift it above shoulder height
weakness in your arm
pain or aching at night, particularly when sleeping on the affected side, which can affect your sleep
Shoulder impingement doesn’t usually cause stiffness so if you have similar symptoms but your shoulder is stiff, you may have another problem such as a frozen shoulder.
When should you get medical help?
The first line of treatment for shoulder impingement should be non-operative. Over the counter pain killers such as an anti-inflammatory can help with pain and inflammation. In addition to pain killers icing the shoulder may help with inflammation. Gently hold an ice pack (or bag of frozen peas) wrapped in a towel on your shoulder for 15 to 20 minutes a few times a day. You can find a good shoulder ice pack here.
Most patients with shoulder pain tend to rest their shoulder to avoid pain and this can quickly lead to weakness of the rotator cuff muscles, so it is important to exercise the shoulder to improve strength and posture for long term control of symptoms.
The British Elbow & Shoulder Society has produced a resource for patients with subacromial shoulder pain. This provides information and a good home exercise program to help rehabilitate the shoulder.
If these self-management options do not work, some patients may go on to need subacromial steroid injections for control of pain and inflammation, and formal exercise focused physiotherapy to work on strength and posture. Patients usually require at least 12 weeks of physical therapy to see long term improvements.
Patients with calcific tendonitis may require slightly different treatment.
What not to do with shoulder impingement?
Avoid things that make the pain worse – avoid activities that involve repeatedly lifting or moving the arm above your head (such as swimming or playing tennis) for a few days or weeks. Heavy lifting and overhead activities such as DIY may aggravate your symptoms so they are best avoided while you undergo treatment.
Do not stop moving your arm completely – try to carry on with your normal daily activities as much as possible so your shoulder does not become weak or stiff. It’s usually best to avoid using a sling.
What if non-operative management does not work?
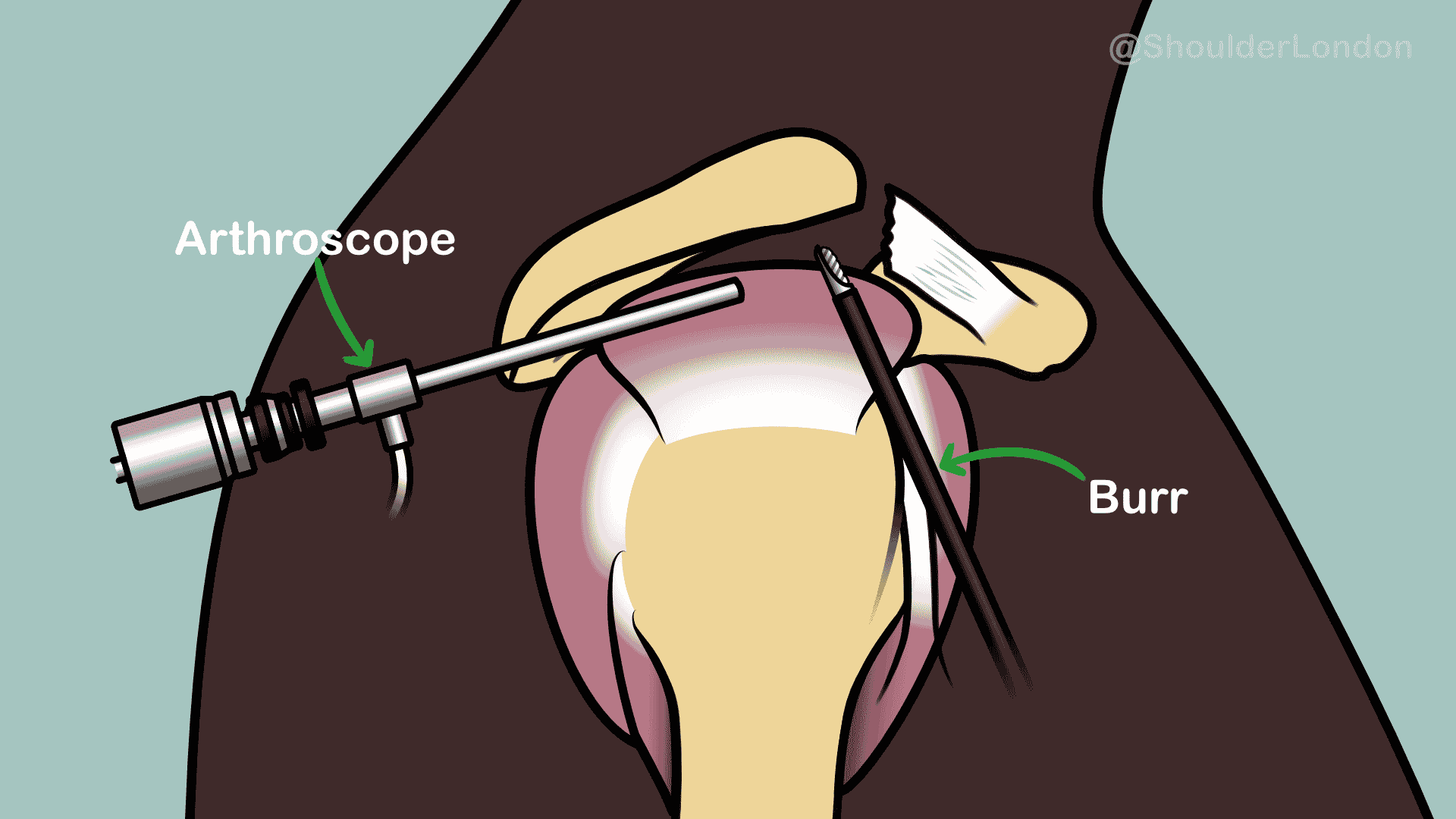
Side view showing bursa removed, spur shaved and ligament released. (Click to Enlarge)
In some patients who fail to improve after steroids and physiotherapy and have persistent pain, surgery may be required. Any surgery required depends on the cause of the pain.
Most patients with persistent shoulder impingement may require an arthroscopic subacromial decompression. This operation is a key-hole, day-case, operation to clear out the subacromial bursa and shave the underside of the acromion and release the coracoacromial ligament in order to increase the space for the rotator cuff tendons to glide. We recommend that this operation is performed with the patient awake under regional anaesthetic. You can find out more about awake shoulder surgery here.